Cricothyrotomy
|
Documentation
Resources:
|
Equipment
Requirements
|
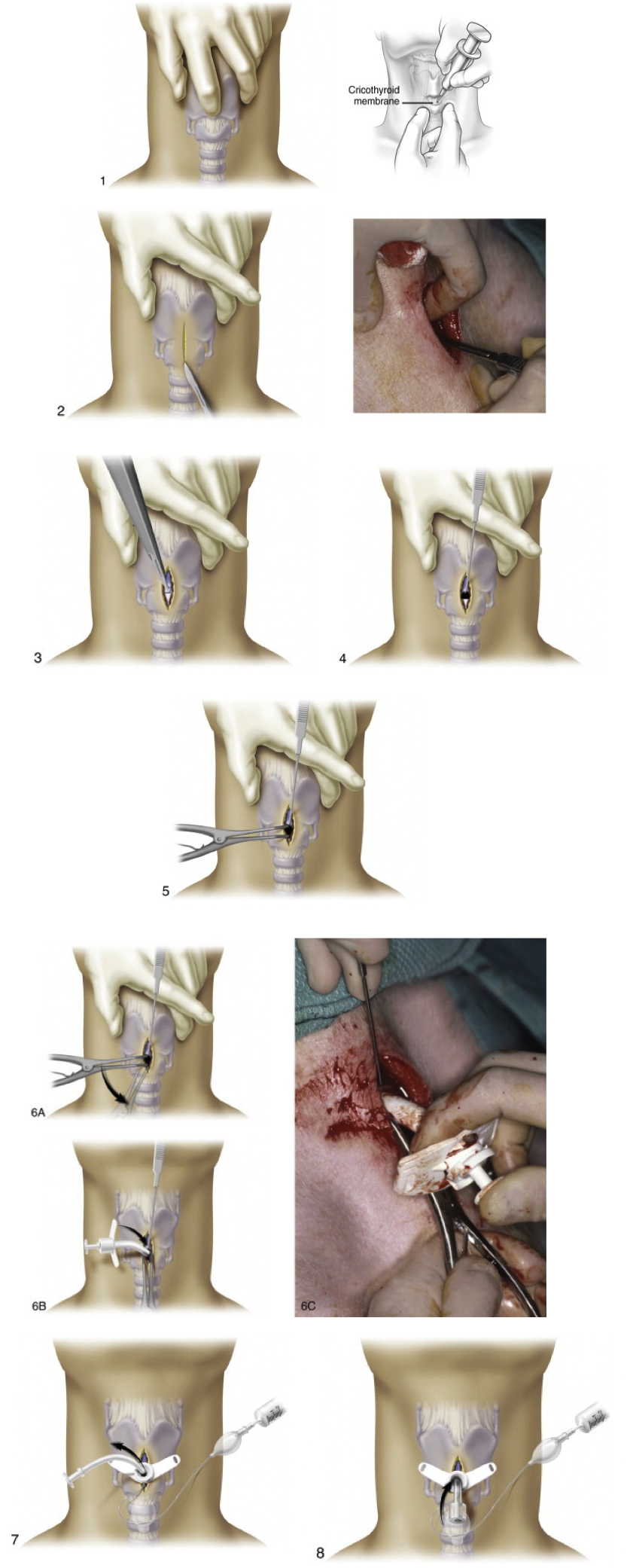
| Procedure: Positioning is crucial
Supine position is ideal Hyperextend the neck if able (i.e. no c spine issues) Preoxygenate with bag valve mask Prepare skin with sterile antiseptic, sterile field and local lidocaine with epi if able Check integrity of balloon on Shiley If right hand dominant stand on patients right side Stabilize larynx with non dominant hand by grasping both sides of lateral thyroid cartilage with thumb and middle finger (throughout the procedure) Palpate depression over cricothyroid membrane with index finger Hold scalpel in dominant hand and make vertical incision through skin and subq Palpate cricothyroid membrane with index of non-dominant hand Remainder of procedure is performed via palpation, as many times bleeding obscures view Make horizontal incision of less than 1 cm through cricothyroid membrane Place non dominant hand index finger into stoma and exchange scalpel for tracheal hook, do NOT let go of stoma Using dominant hand place hook into the opening of the cricothyroid membrane and grasp the inferior of the thyroid cartilage with it Rotate handle cephalad and if an assistant is present ask for upward traction (or by self using non dominant hand) Do not let go of tracheal hook until rest of procedure is complete as this stabilizes the larynx Place trousseau dilator in hole with dominant hand with spreading action oriented in longitudinal direction and Dilate vertically Rotate handle 90 degrees so handle is parallel to neck Insert tracheal tube with obturator (solid white piece) between blades of dilator until flanges rest on skin Remove hook carefully (after balloon inflated) Rapid Four Step Technique: If right hand dominant, stand at the bedside on the patients left side
Kit, like central line |
 |
Procedure
Note:
Date:
Indication: emergency airway
Resident:
Attending:
Consent was obtained and a time-out was completed verifying correct patient, procedure, site, and positioning. The patient’s neck was prepped and draped in sterile fashion. 1% Lidocaine was(?)was not used to anesthetize the surrounding skin area. The cricothyroid membrane was palpated. The skin over the cricoids membrane was incised with a scalpel. The cricothyroid membrane was subsequently incised and the inferior thyroid cartilage. The cricothyroid membrane was dilated and a tracheal tube with obturator (or Endotracheal tube) was placed in the incision site. The patient tolerated the procedure well and there were no complications. Blood loss was minimal.
Chest x-ray was(?)was not ordered to assess for pneumothorax and proper placement.
Date:
Indication: emergency airway
Resident:
Attending:
Consent was obtained and a time-out was completed verifying correct patient, procedure, site, and positioning. The patient’s neck was prepped and draped in sterile fashion. 1% Lidocaine was(?)was not used to anesthetize the surrounding skin area. The cricothyroid membrane was palpated. The skin over the cricoids membrane was incised with a scalpel. The cricothyroid membrane was subsequently incised and the inferior thyroid cartilage. The cricothyroid membrane was dilated and a tracheal tube with obturator (or Endotracheal tube) was placed in the incision site. The patient tolerated the procedure well and there were no complications. Blood loss was minimal.
Chest x-ray was(?)was not ordered to assess for pneumothorax and proper placement.