Pericardiocentesis
|
Documentation
|
Equipment
Requirements
|
| Procedure: General:
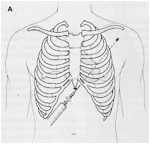
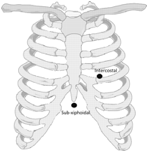
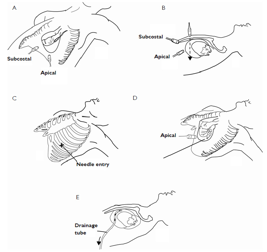
If time permitting, use lidocaine 1-2% If time permits: elevate the chest to 45 degree angle, and decompress abdomen if distended 16-18 gauge needle, 5-8 cm in length is ideal Attach a saline filled syringe and gently aspirate as needle advanced You can inject agitated saline once pericardial space is entered to confirm placement (can also check EKG for ST elevations, than 2 far and need to withdraw) After confirmation, pass a wire through the sheath and use a 6-8 French dilator Pass an introducer over the wire after dilator is removed (6-8 French) (just like central line kit) Remove sheath and wire and leave cordis in place Subxiphoid view: Place probe in transverse plane at left costal margin at point of xyphoid process and aim to left shoulder Parasternal view: Place transducer in left parasternal area between second and fourth intercostals space Blind Pericardiocentesis:
Anterior chest approach is preferred (reduced risk of liver damage) Also reduced risk for lung puncture (air (lung) obscures fluid so would not see fluid if going through lung) Stay away from internal mammary arteries (3-5 cm from parasternal border) and neurovascular bundles under ribs Complications: |
   |
Procedure Note:
Date:
Indication: Diagnostic/therapeutic removal of fluid from the pericardial space
Resident:
Attending:
Consent was obtained and a time-out was completed verifying correct patient, procedure, site, and positioning. The patient’s thorax was prepped and draped in sterile fashion. 1% Lidocaine was used to anesthetize the surrounding skin area. Ultrasound was(?)was not used to identify the fluid and observe the needle entering the pericardial space. The needle was introduced into the pericardial space. Appropriate fluid return was obtained and fluid was(?)was not removed for study. The needle was then removed. The patient tolerated the procedure well and there were no complications. Blood loss was minimal.
Chest x-ray was performed to assess for pneumothorax.
Date:
Indication: Diagnostic/therapeutic removal of fluid from the pericardial space
Resident:
Attending:
Consent was obtained and a time-out was completed verifying correct patient, procedure, site, and positioning. The patient’s thorax was prepped and draped in sterile fashion. 1% Lidocaine was used to anesthetize the surrounding skin area. Ultrasound was(?)was not used to identify the fluid and observe the needle entering the pericardial space. The needle was introduced into the pericardial space. Appropriate fluid return was obtained and fluid was(?)was not removed for study. The needle was then removed. The patient tolerated the procedure well and there were no complications. Blood loss was minimal.
Chest x-ray was performed to assess for pneumothorax.